


ABSTRACT
The operating room environment is very dynamic with many unique challenges for anesthesia teams caring for patients with confirmed or suspected COVID-19. Specific recommendations by national organizations and institution specific step-by-step guidelines and education materials are required to maintain safety for both patients and caregivers perioperatively, with transport, and medication management.
INTRODUCTION
Anesthesiology caregivers face new challenges in perioperative areas and the operating room (OR) in caring for patients with COVID-19 and patients under investigation (PUI) for COVID-19.
In addition to recommendations issued by national organizations such as the Centers for Disease Control and Prevention, the Anesthesia Patient Safety Foundation1 and the American Society of Anesthesiology,2 the Anesthesiology Institute at Cleveland Clinic has created step-by-step guidelines for patients with COVID-19 and PUI for COVID-19 requiring surgery or procedures with anesthesia. Key considerations are shared below.
PREOPERATIVE
Before the patient arrives in the OR, the entire OR team should perform a huddle to discuss the logistics of the patient transportation, procedure, and disposition.
Monitored anesthesia care or regional anesthesia should be avoided and general anesthesia should be considered for patients with confirmed or suspected COVID-19.
All equipment and medication need to be prepared in advance, so patients can be brought directly to the OR and induced (if not intubated) without delay.1 Patients who are in the intensive care unit (ICU), but not intubated should preferably be intubated in the ICU by the anesthesia team before transport to the OR.
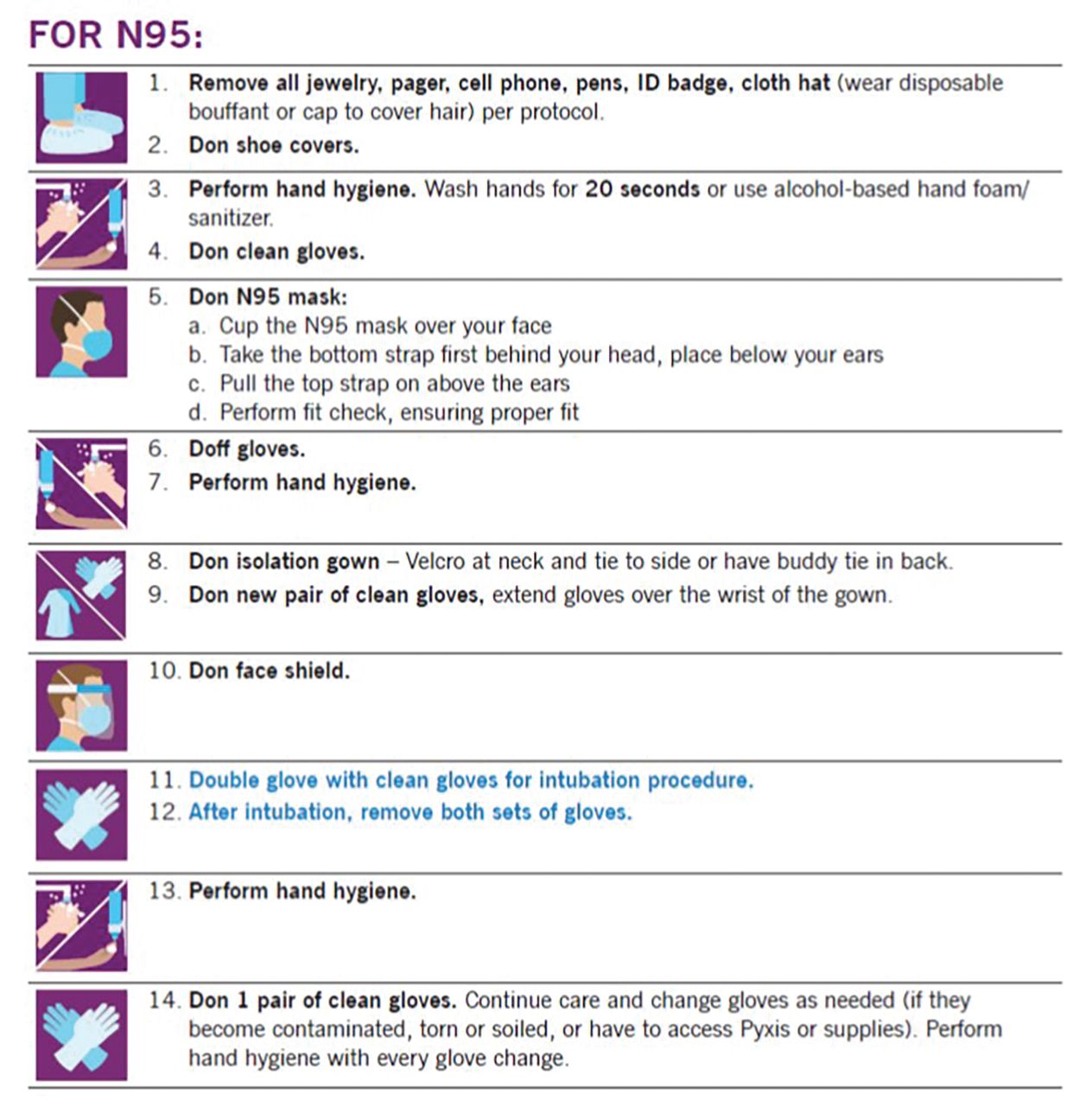
In preparation for intubation, anesthesia team members should properly don personal protective equipment (PPE) using the buddy system. There are specific considerations for use of PPE based on American Society of Anesthesiology recommendations such as double gloving for intubation2 (Figure 1).

Personal protective equipment donning protocol (N95 users) for anesthesia providers taking care of patients with confirmed or suspected COVID-19.
The member of the anesthesia team with the most experience intubating patients should perform the intubation and the number of caregivers near the patient should be minimized. Measures to decrease the chance of aerosolization and contamination should be implemented (ie, barrier device over the patient’s head, no bag-mask ventilation, rapid sequence induction, use of video-laryngoscopy).
Proceeding with rapid sequence induction is recommended,2,3 try to avoid Fentanyl, to prevent coughing consider the use of Esmolol or Lidocaine or both. Once the patient is unconscious, the patient should be covered with a plastic transparent drape/barrier device, while maintaining intubating equipment and suction visible underneath it. Bag-mask ventilation of the patient should be avoided. However if, manual ventilation is needed, small tidal volumes with two-handed mask ventilation to ensure good mask seal should be utilized.
Video laryngoscope for intubation is preferred. Once the patient is intubated, the endotracheal tube cuff needs to be inflated. Connect to heat and moisture exchanger filter and anesthesia circuit, initiate ventilation. Check for presence of end-tidal carbon dioxide (ETCO2) and bilateral chest rise. With all the PPE in place, auscultating the patient may not be the best way to confirm proper position of the endotracheal tube. Checking for endotracheal tube depth, chest rise, and ETCO2 is a better choice.
Once intubation is successful, the patient should be adequately sedated (with sedatives and muscle relaxant) and stable for transport. Providers who participated in intubation should change below-the-neck PPE using the buddy system.
INTRAOPERATIVE
Patients either from the ICU or other locations should be brought directly into the OR and universal protocol for safety check should be followed.
If the patient is on supplemental oxygen, oxygen flow should be maintained at minimum necessary to decrease the potential for aerosol generation. They should keep their protective isolation mask on right up to the induction of anesthesia, and only uncover for the anesthesia team’s airway exam. Perform a meticulous airway assessment as this may be your first opportunity to assess the patient’s uncovered airway.
OR preparedness is fundamental.3,4 Make sure to have a video laryngoscope with transparent plastic cover, empty biohazard plastic bags available to dispose of used blades when contaminated, styletted endotracheal tubes, precut tape straps or tube strap to secure the endotracheal tube once in place. Additionally, have available airway backup devices like a laryngeal mask airway, a disposable laryngoscope, a bougie, oral and nasopharyngeal airways.
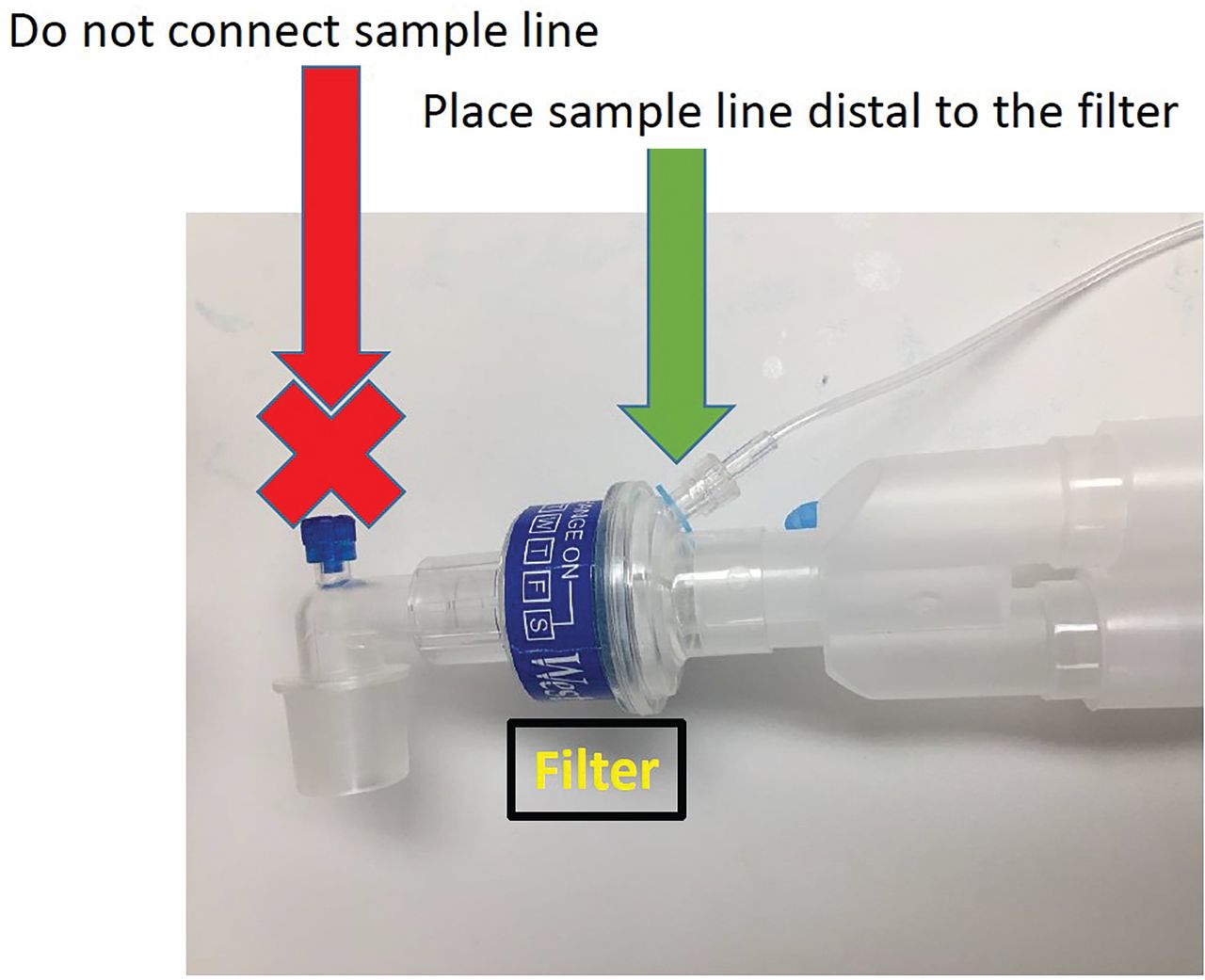
It is fundamental that the heat and moisture exchanger filter is in place at the distal end of the anesthesia circuit Y-piece, with an ETCO2 monitor in the protected side of the circuit, this will help filter the patient’s exhaled breaths (Figure 2).

Use of heat and moisture exchanger filter on anesthesia machine and appropriate placement on the anesthesia circuit. Place filter proximally between the mask and patient limb of the circuit and place a second filter between expiratory limb and machine.
As you are getting ready for induction, place all medications on a designated table including emergency medications. Personnel nonessential to induction should leave the room.
Before you proceed with induction, make sure you put on a second pair of gloves. If inducing a nonintubated patient in the OR, you should follow above mentioned induction procedures. Resheath the laryngoscope immediately postintubation. Seal all used airway equipment in a double zip-locked plastic bag. Once settled, remove your gloves, perform hand hygiene, and put on a single new pair of gloves.
Remember to place the ventilator on standby whenever a circuit disconnection is required, such as tube repositioning, and to restart mechanical ventilation only after the circuit has been reconnected.
Any contact with outside personnel for supplies, blood products, and samples should be minimized. It is advised to have at least 1 dedicated runner to assist the anesthesia team.
POSTOPERATIVE
If extubation is planned, all members of the surgical team not required should leave the room. Once you deem the patient is ready for extubation, place plastic transparent drape/protective devices over the patient and proceed with extubation, while utilizing strategies to prevent coughing. Make sure to keep the anesthesia face mask tightly fitted to the patient’s face when the patient coughs. Once stable, place a nasal cannula/oxygen face mask and a surgical face mask to cover the patient’s airway. Remove plastic transparent drape/protective devices.
Extubated patients and those who undergo procedures under a regional anesthetic can be recovered in the OR. Other than ICU patients, after phase II recovery criteria are met, patients can be transported back to their designated hospital rooms.
In preparation for patient transport by a 2-member anesthesia team, each member changes below-the-neck PPE using the buddy system in sequence, such that at least 1 anesthesia team member monitors the patient in the OR at all times.
After communicating with the receiving team on the floor or ICU, both members of the anesthesia team should transport the patient.
Once handoff communication is complete between the OR and floor or ICU receiving team, PPE can be removed using the buddy system outside the patient room. Ensure that all contaminated and disposable equipment including protective gear and medications are disposed appropriately. Unused, uncontaminated medications can be returned to the OR electronic medicine cabinet system. All nondisposable and contaminated or potentially contaminated objects such as monitors, cables, and anesthesia machine are cleaned with the recommended disinfectants.
SPECIAL CONSIDERATIONS
Transport
The transport from the ICU to the OR needs to be carefully choreographed, with a designated runner who can ensure effective logistics, such as clear hallways, elevator, access to surgical area, opening OR doors, and preventing cross contamination. For patients on ongoing mechanical ventilation, circuit or resuscitator disconnections are guarded against disconnection during transport.
Medication management
To minimize waste, remove only the volume of medications that might be needed for the case. For medications that you want to have on standby in case of an emergency, remove and place them in a clean, sealed plastic bag. These can be returned to the medication cabinet at the end of the case if they are not opened or contaminated.
The medication cabinet remains open in the room during cases and the exterior is cleaned after the case ends.4 If the medication cabinet or the sealed plastic bag containing emergency medications needs to be accessed after contact with the patient, perform hand hygiene and don a new pair of gloves remove the medication.
Footnotes
The statements and opinions expressed in COVID-19 Curbside Consults are based on experience and the available literature as of the date posted. While we try to regularly update this content, any offered recommendations cannot be substituted for the clinical judgment of clinicians caring for individual patients.
- Copyright © 2020 The Cleveland Clinic Foundation. All Rights Reserved.
In this issue




{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.