


Article Figures & Data
Figures
- Figure 1
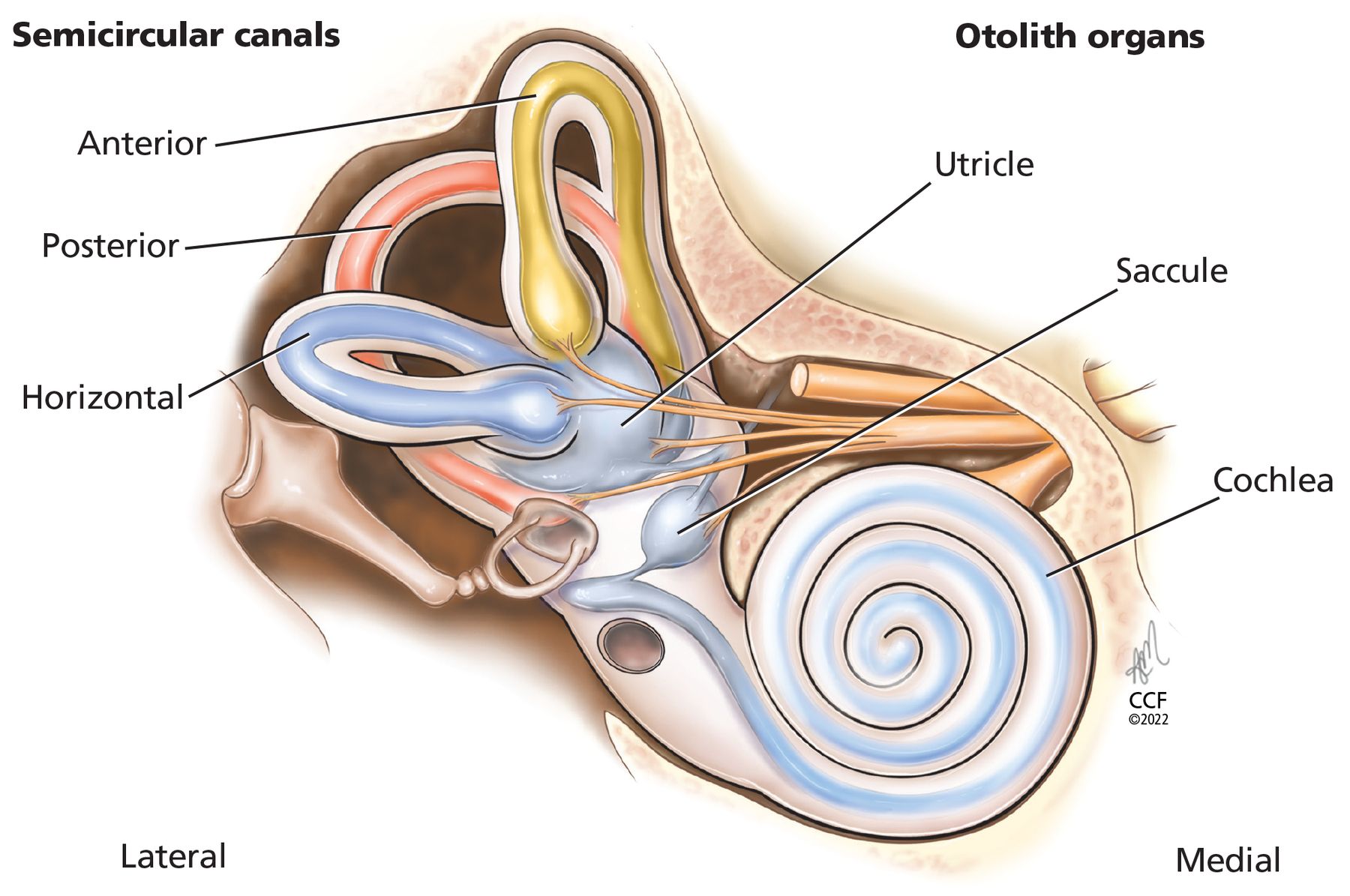
The semicircular canals (anterior, posterior, horizontal) sense angular acceleration, and the otolith organs (saccule, uticle) sense linear acceleration, providing internal cues for orientation of position in space, movement, gaze stabilization, and postural control.
- Figure 2
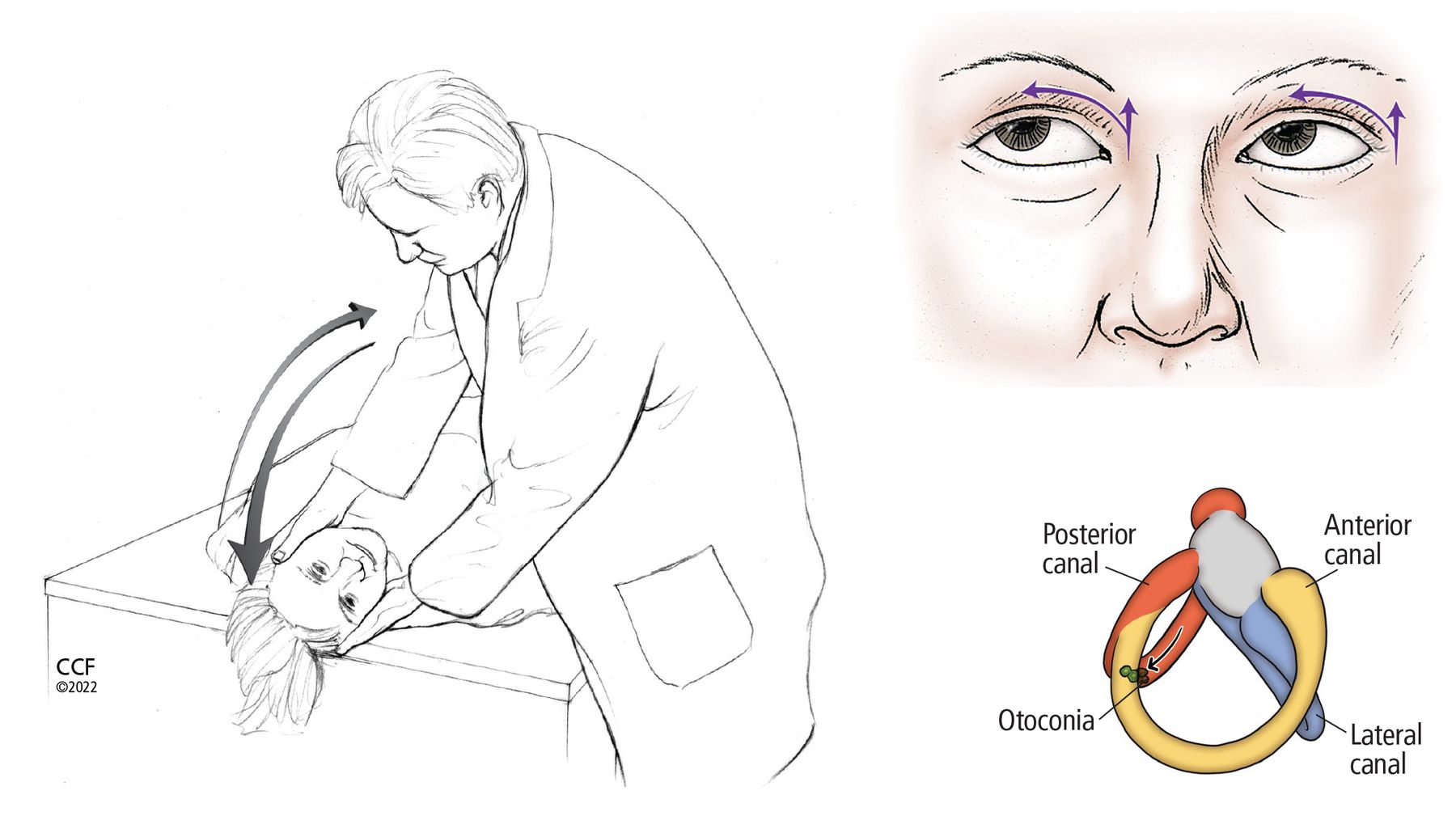
The Dix-Hallpike maneuver to detect otoconia in the posterior or anterior semicircular canals. If the otoconia are suspected to be in the right ear, the patient sits upright with the head turned 45° to the right; if the otoconia are suspected to be in the left ear, the patient turns the head to the left. The clinician then quickly moves the patient into a head-hanging supine position and checks for signs of nystagmus, and the patient reports any symptoms (eg, dizziness, vertigo). After 60 seconds, the patient is returned to a seated position with the head still turned, and the clinician again observes symptoms and signs. During the maneuver, movement of otoconia within the right posterior semicircular canal (in the lower-right image) causes an excitatory response—ie, nystagmus—to the right and up, as the arrows indicate in the upper-right image.
- Figure 3
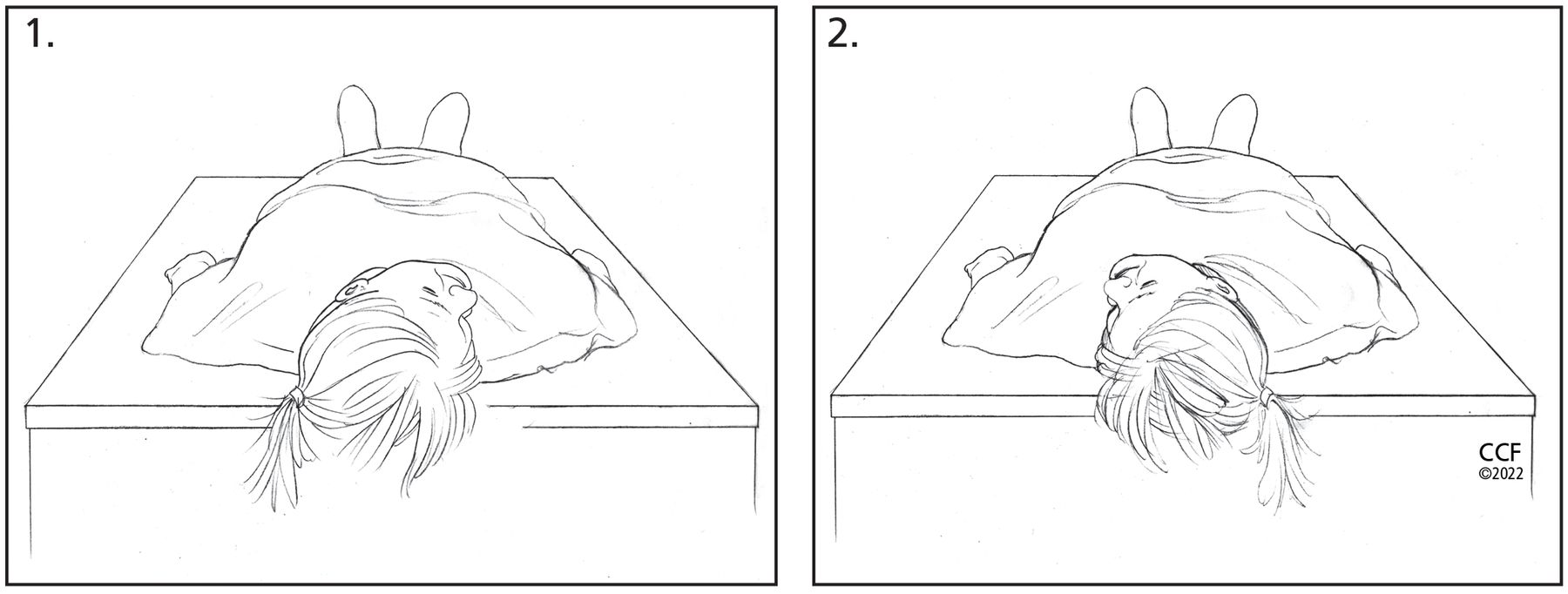
The supine roll test to detect otoconia in the horizontal semicircular canals. (A) With the patient in a supine position, the clinician quickly rotates the patient’s head to the right and assesses for horizontal nystagmus and patient symptoms. (B) After 30 to 60 seconds, the clinician quickly rotates the patient’s head to the left and again observes for horizontal nystagmus and symptoms. The direction of nystagmus (ie, geotropic vs apogeotropic) with the head-movement changes indicates the involved horizontal canal (Table 2).
- Figure 4
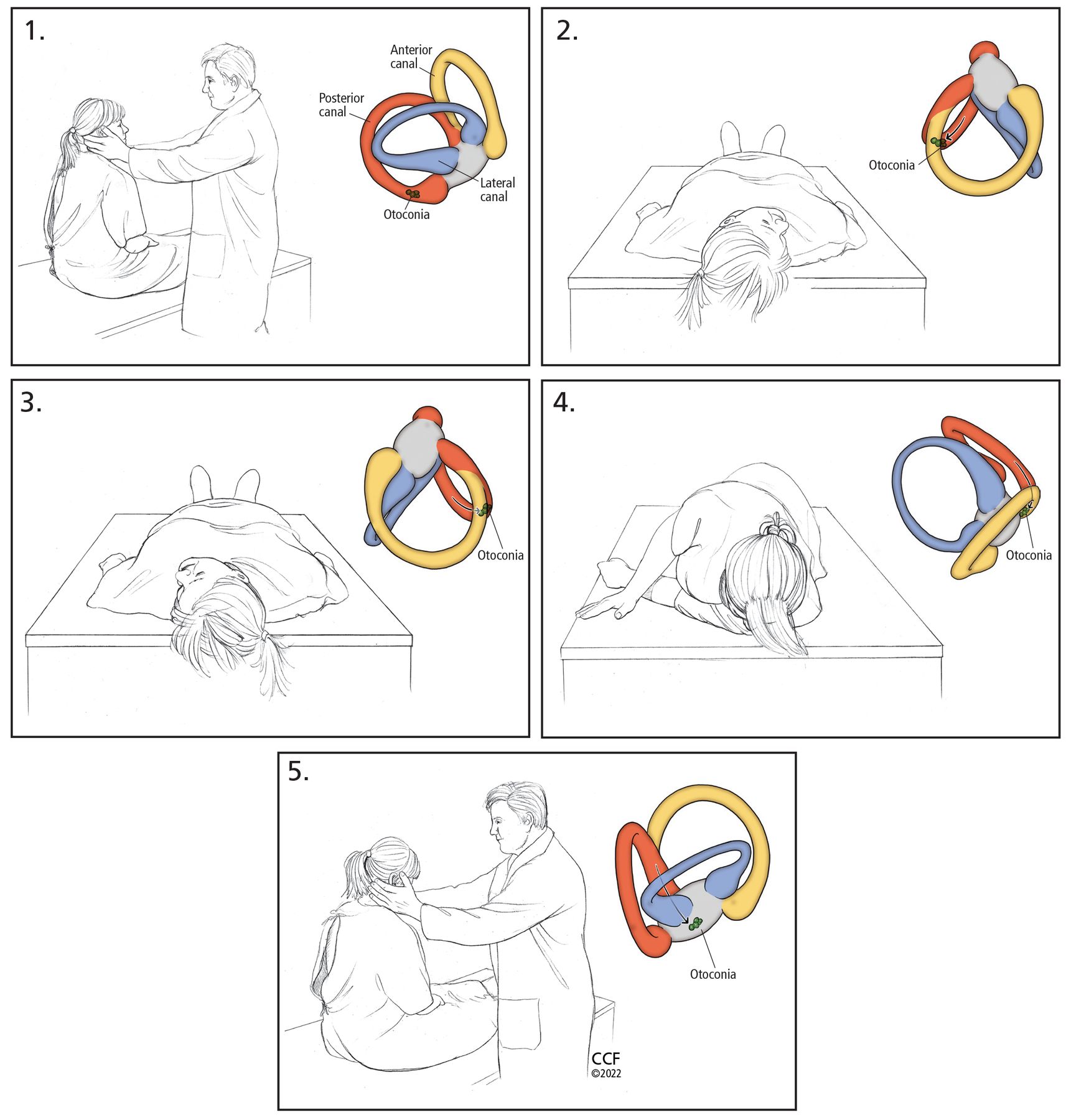
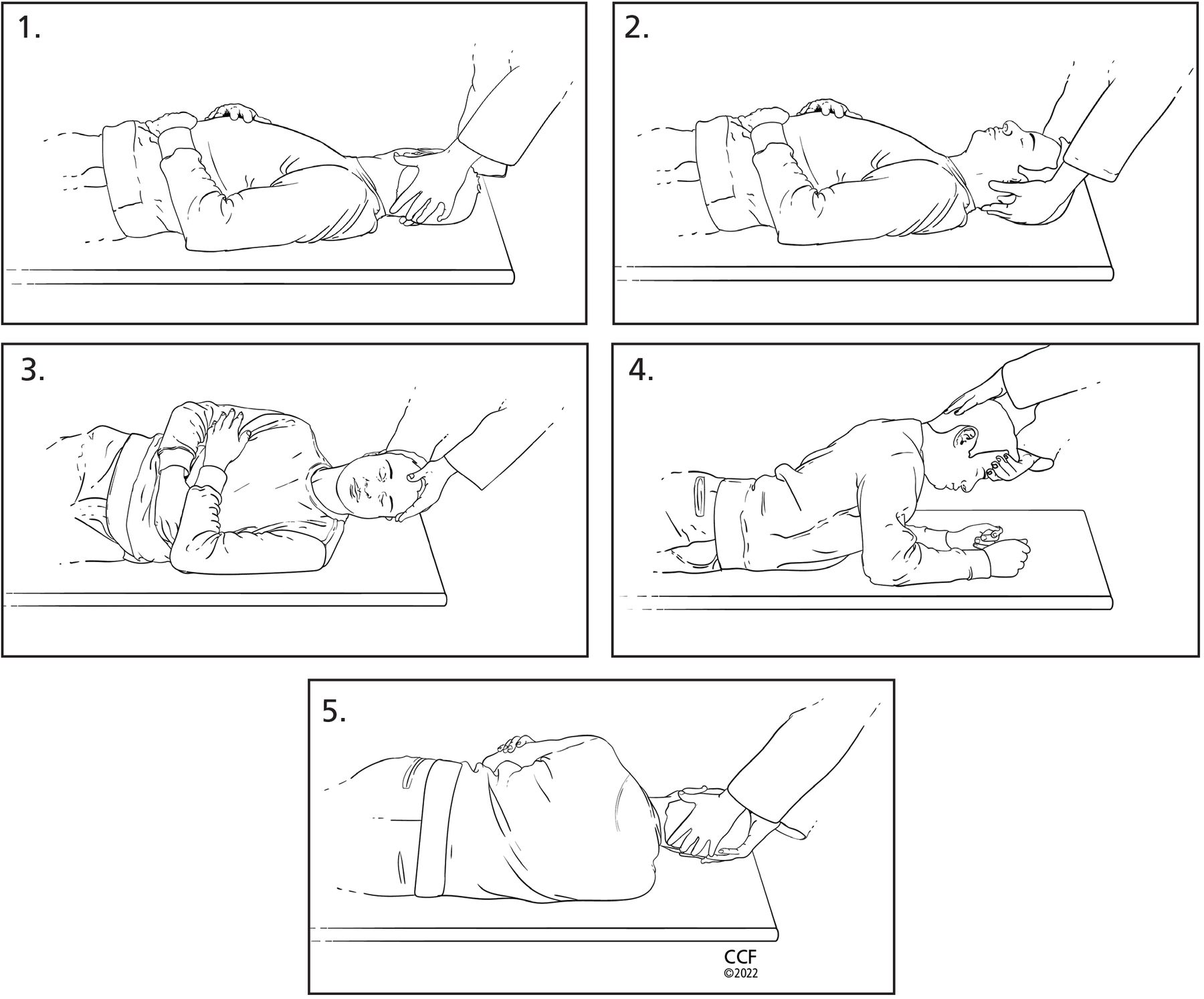
The Epley maneuver to clear otoconia from the posterior or anterior semicircular canals:
Place the patient in a seated position on the bed and turn their head 45° toward the ear with the suspected otoconia. The color insets show movement of otoconia.
Quickly move the patient to a supine position with head turned and extended downward.
Move the patient’s head to the other side, being careful to keep it in the correct plane. The final position after turn should be 45° toward the unaffected ear, extended downward.
Assist the patient onto the unaffected side with the patient’s chin remaining 45° toward the unaffected ear (patient will be looking toward the ground in this position).
Finally, help the patient back to a seated position, keeping their head turned over their shoulder.
- Figure 5
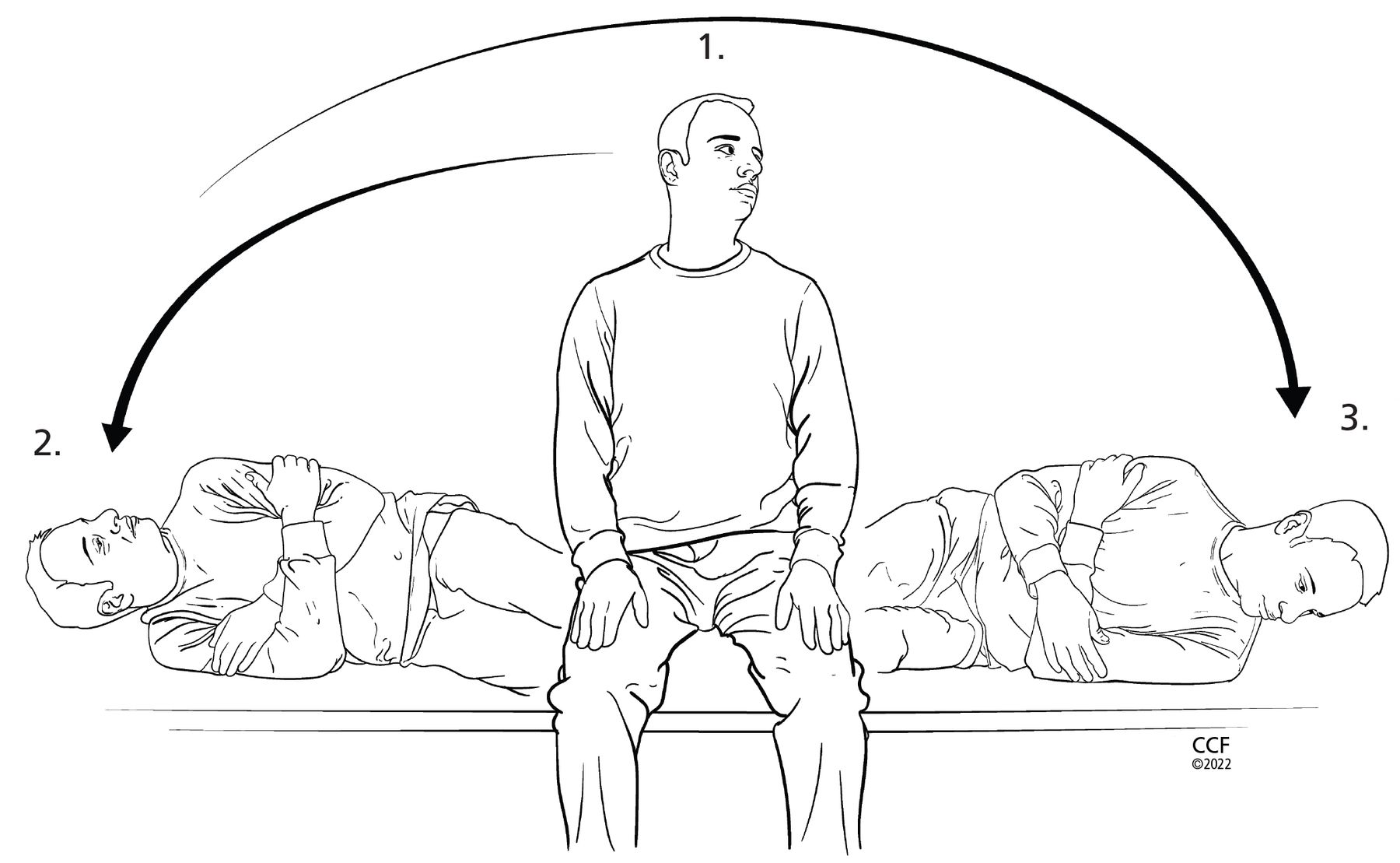
Semont maneuver, an alternative way to clear otoconia from the posterior or anterior canals:
Place the patient in a seated position on the bed and turn the head 45° away from the ear with the suspected otoconia in the vertical semicircular canal.
Quickly move the patient on their side with the nose facing the ceiling.
Quickly move the patient back up and onto their other side with the head in the same 45° angle with the nose facing toward the ground. The examiner then assists the patient to a seated position, keeping the head at 45° away from the ear with suspected vertical semicircular canal benign paroxysmal positional vertigo (BPPV).
Note: The head position described in step 1 is used for posterior semicircular canal BPPV. The patient should turn the head 45° toward the ear with suspected vertical semicircular canal BPPV if the anterior semicircular canal is affected.
- Figure 6
Log roll (360°) maneuver to clear otoconia from the horizontal semicircular canal:
Place the patient in the supine position and turn their head 90° toward the ear with the suspected otoconia in the horizontal semicircular canal.
Next, turn the patient’s head back to center, with the head elevated 30°.
Maneuver the patient onto their side (90°) toward the unaffected ear.
Move the patient into the prone position with elbows flexed. Note: Sometimes treatment can end in this position (called 270° maneuver).
Finally, help the patient back onto their back toward the ear involved, completing a complete 360° rotation.






Tables
Disorder Symptoms Temporal pattern Benign paroxysmal positional vertigo (BPPV) Head or body movement-provoked vertigo Episodic; seconds to minutes; can have delayed latency in symptoms or fatigue of symptoms upon repeat movement Cervical vertigo Dizziness, imbalance or lightheadedness with neck pain or changes in neck position Episodic; minutes to hours Menière disease Vertigo with fluctuating hearing loss, aural fullness, and tinnitus Spontaneous onset; episodic; 20 minutes to 24 hours Vestibular neuritis Vertigo without auditory symptoms, followed by head movement-provoked symptoms Sudden onset; 1–3 days Labyrinthitis Vertigo with auditory symptoms, followed by head movement-provoked symptoms Sudden onset; several days Acoustic neuroma or vestibular schwannoma Imbalance with brief episodes of dizziness; auditory symptoms; occasional neurologic symptoms Gradual onset; progressive and continuous Superior canal dehiscence Autophony, disequilibrium, positional vertigo, and pressure- or sound-induced symptoms of vertigo Episodic; seconds to minutes Perilymphatic fistula Pressure- or sound-induced symptoms of vertigo, imbalance Sudden onset; episodic; seconds to minutes Vascular event (anterioinferior cerebellar artery or posterioinferior cerebellar artery stroke) Vestibular crisis event: vertigo with associated hearing loss and other neurologic symptoms and signs followed by head movement-provoked symptoms Sudden onset; lasting 1–3 days Based on information in references 3 and 4.
Provocative maneuver Nystagmus direction Affected canal Dix-Hallpike To the affected side and up Posterior Dix-Hallpike To the affected side and down Anterior Supine roll, right ear down
Supine roll, left ear downRight (geotropic)
Left (geotropic)Horizontal. The head-turn direction eliciting stronger nystagmus indicates the affected horizontal canal Supine roll, right ear down
Supine roll, left ear downLeft (apogeotropic)
Right (apogeotropic)Horizontal. The head-turn direction eliciting weaker nystagmus indicates the affected horizontal canal Location Treatment maneuver Posterior canal Epley or Semont Anterior canal Epley or Semont Horizontal canal (geotropic-type nystagmus pattern) Log roll (360°)




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}