


Article Figures & Data
Figures
- Figure 1
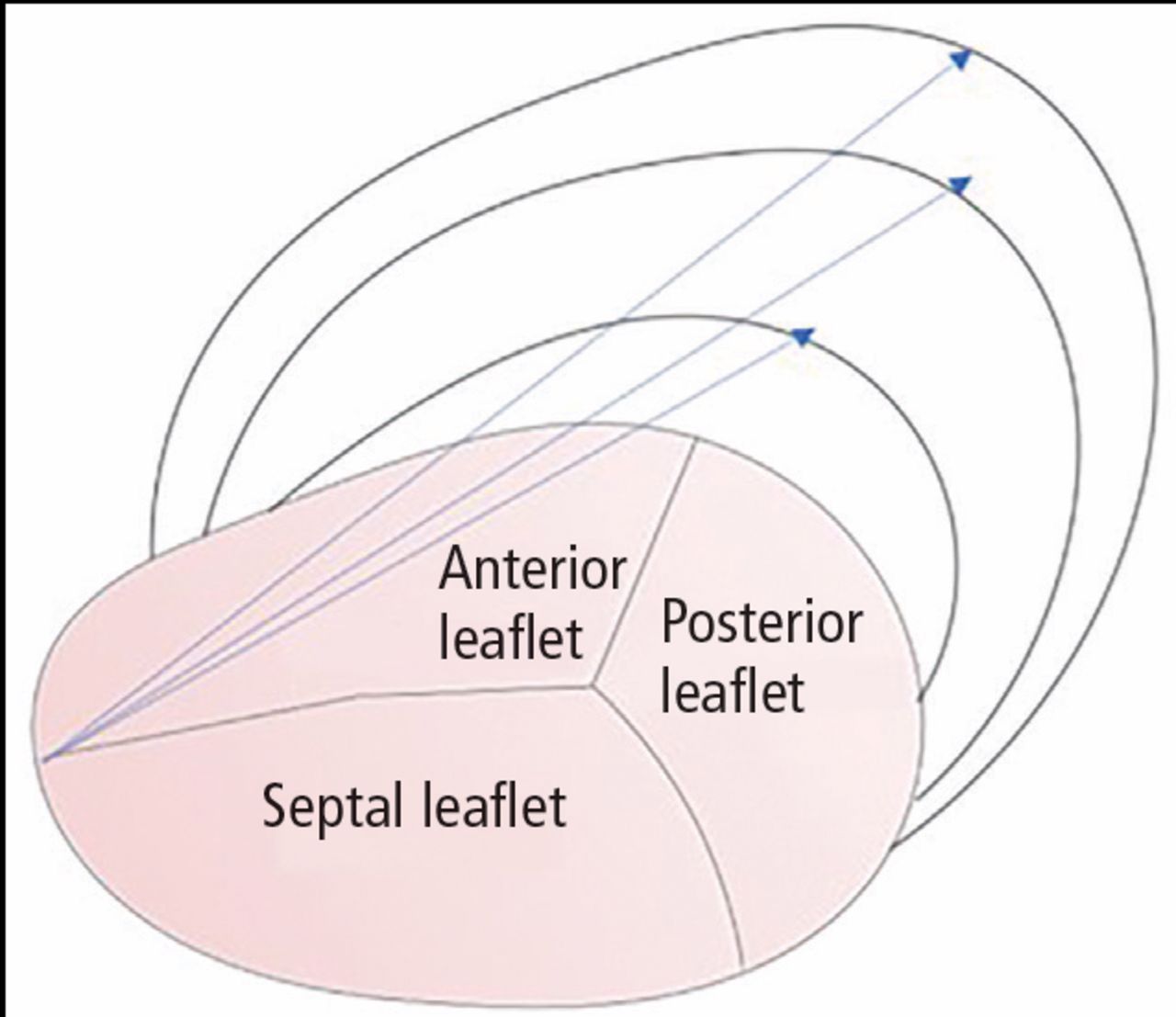
Schematic representation of the anatomy of the tricuspid annulus. The arrows represent annular dilation resulting in an increased anteroposterior diameter in functional tricuspid regurgitation.
- Figure 2
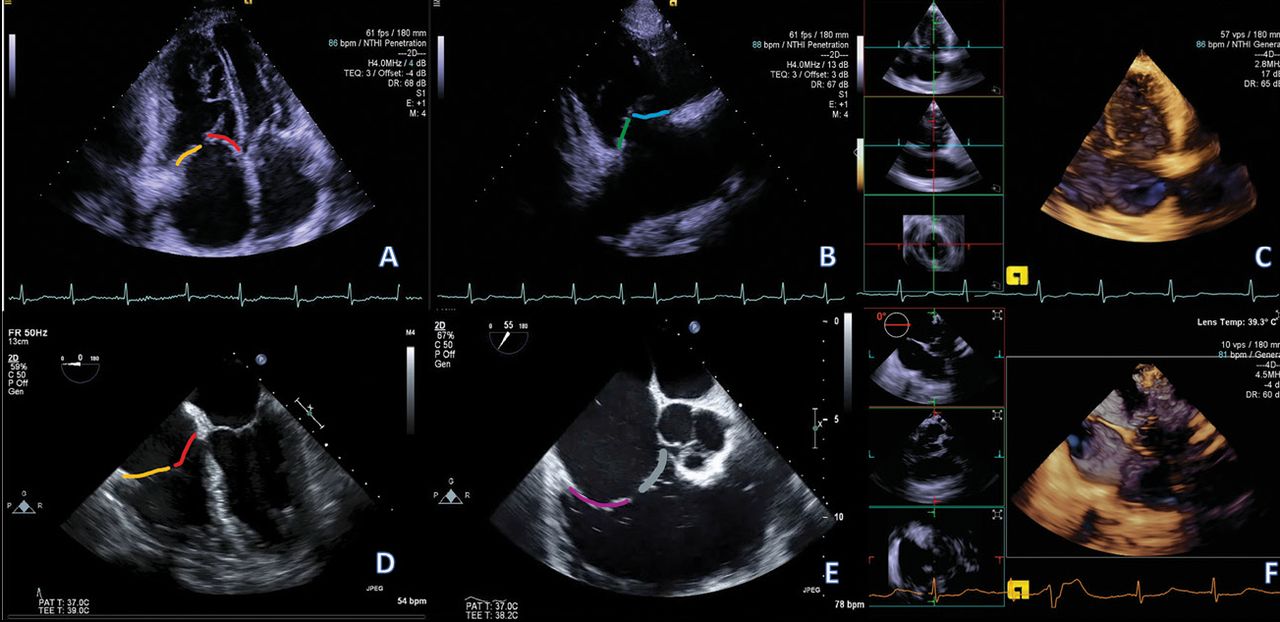
(A–C) Transthoracic echocardiography (TTE) views and (D–F) transesophageal echocardiography (TEE) views of the tricuspid valve (TV). (A) TTE 4-chamber view: The septal leaflet is shown in red. The other leaflet (orange) could be the anterior leaflet (if probe is angled anteriorly and the aortic valve is brought into view, ie, 5-chamber view) or the posterior leaflet (if probe is angled posteriorly and coronary sinus brought into view). (B) TTE RV inflow view: The anterior leaflet is shown in blue. The other leaflet (in green) could be the posterior leaflet or the septal leaflet. (C) TTE 3D focused on the tricuspid valve. Three orthogonal planes centered on the TV are cross-referenced (inlets on the left), allowing easier identification of the different leaflets. (D) TEE 4-chamber view: As in the TTE 4-chamber view, the septal leaflet (in red) is identified, and the other leaflet (orange) could be either the anterior or posterior. (E) TEE RV inflow view: The posterior leaflet is shown in purple, the other leaflet (in grey) could be either the anterior or septal leaflet. (F) TEE 3D focused on the tricuspid valve. As in the 3D TTE, 3 orthogonal planes are cross-referenced. The different leaflets are easier to identify.
- Figure 3
(A and B) Steady-state free precession magnetic resonance images in a 4-chamber and short-axis orientation, respectively. (A) Severely dilated tricuspid annulus (double arrow in yellow). The arrow in D points to a large area of central regurgitation (flow dephasing) caused by a lack of leaflet coaptation secondary to severe annular dilation. (C) Corresponding computed tomography image in a 4-chamber orientation also demonstrating an enlarged annulus (double arrow in yellow). The annular enlargement is better appreciated on the short-axis view (D, blue arrows).
- TABLE 1
Staging of functional tricuspid regurgitation
- Figure 4
MitraClip.
- Figure 5
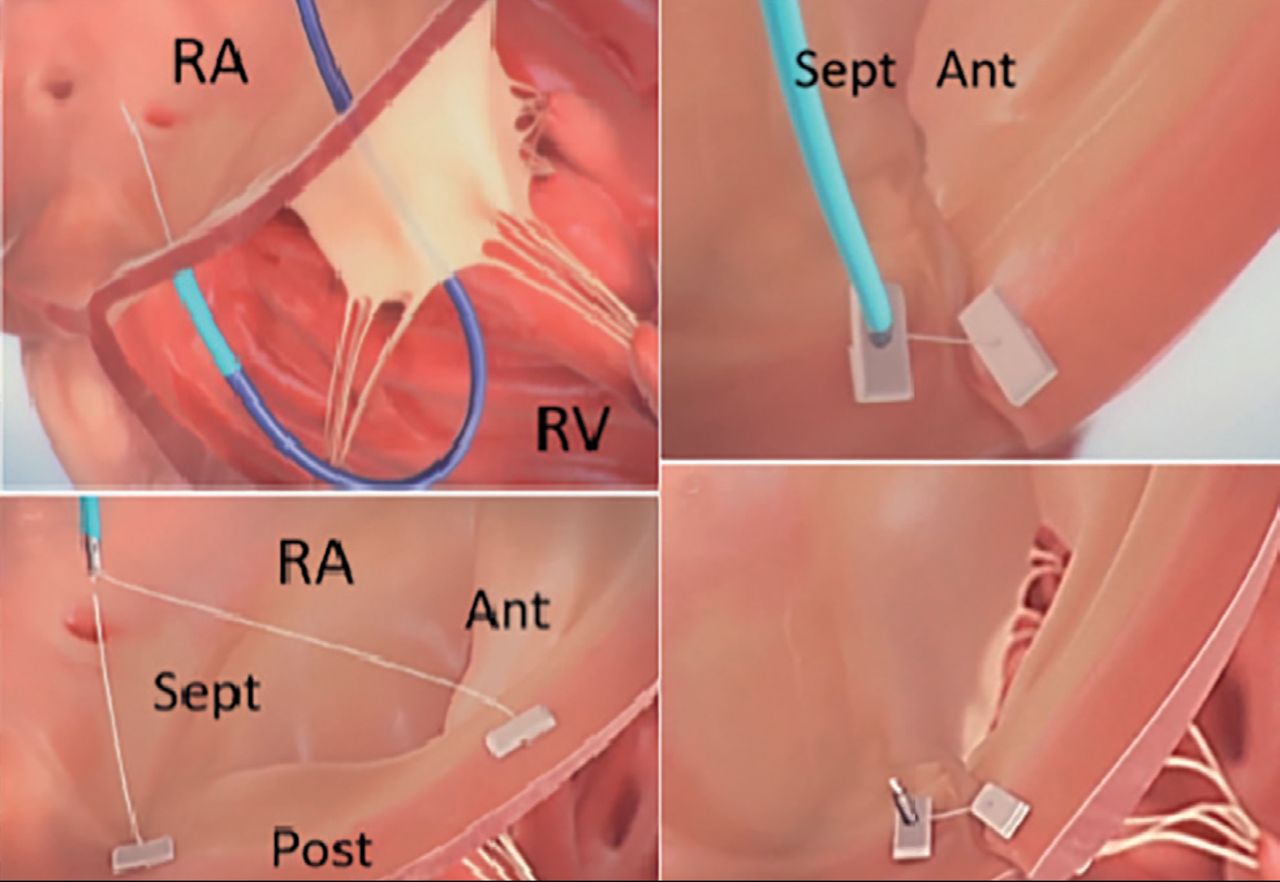
TriAlign system.
Ant = anterior; Post = posterior; RA = right atrium; RV = right ventricle; Sept = septal
Source: SCOUT study video from HeartValveSurgery.com
- Figure 6
Gate valve.







Tables
Mild Moderate Severe Massive Torrential Central jet area < 5 cm2 5–10 cm2 > 10 cm2 Vena contracta (biplane) < 3 mm 3–6.9 mm 7–13 mm 14–20 mm ≥ 21 mm EROA (PISA) < 20 mm2 20–39 mm2 40–59 mm2 60–79 mm2 ≥ 80 mm2 Vena contracta width Not defined < 0.70 cm > 0.70 cm Continuous wave jet density and contour Soft and parabolic Dense and variable Dense, triangular with an early peak Hepatic vein flow Systolic dominance Systolic blunting Systolic reversal Cardiac chambers and IVC Normal size of RA/RV/IVC No RV enlargement, no or mild RA enlargement, no or mild IVC enlargement with respirophasic variation. Normal RA pressure. RV/RA/IVC dilated with decreased IVC respirophasic variation. Elevated RV pressure. Diastolic intraventricular septum flattening. Reduced RV systolic function in late phase. 3D VCA or quantitative EROA 75–94 mm2 95–114 mm2 ≥ 115 mm2 3D VCA = three-dimensional vena contracta area; EROA = effective regurgitant orifice area; IVC = inferior vena cava; PISA = proximal isovelocity surface area; RA = right atrium; RV = right ventricle
Source: Data from references 1 and 12.
American College of Cardiology/American Heart Association (2014)1 European Society of Cardiology (2017)20 • Tricuspid valve surgery is recommended for patients with severe tricuspid regurgitation (stages C and D) undergoing left- sided valve surgery (Class I, level of evidence C). • Surgery is indicated in patients with severe secondary tricuspid regurgitation undergoing left-sided surgery (Class I, level of evidence C). • Current guidelines provide for tricuspid valve repair in patients with mild, moderate, or greater functional tricuspid regurgitation at the time of left-sided surgery with either tricuspid annular dilation or prior evidence of right heart failure (Class IIa, level of evidence B). • Surgery is indicated in patients with mild or moderate secondary tricuspid regurgitation with a dilated annulus (≥ 40 mm or > 21mm/m2 by 2-dimensional transthoracic echocardiography) undergoing left-sided surgery (Class IIa, level of evidence C). • Tricuspid valve repair may be considered for patients with moderate functional tricuspid regurgitation and pulmonary hypertension at the time of left-sided surgery (Class IIb, level of evidence C). • Surgery may be considered in patients undergoing left-sided surgery with mild or moderate secondary tricuspid regurgitation even in the absence of annular dilation when previous right- sided heart failure has been documented (Class IIb, level of evidence C). • Reoperation for isolated tricuspid valve repair or replacement may be considered for persistent symptoms due to severe tricuspid regurgitation (stage D) in patients who have under- gone previous left-sided valve surgery and who do not have severe pulmonary hypertension or significant right ventricular systolic dysfunction (Class IIb, level of evidence C). • After previous left-sided surgery and in the absence of recurrent left-sided valve dysfunction, surgery should be considered in patients with severe tricuspid regurgitation who are symptomatic or have progressive right ventricular dilation/dysfunction, in the absence of severe left ventricular/right ventricular dysfunction or pulmonary vascular disease/hypertension (Class IIa, level of evidence C). Device Clinical trial (NCT#) Primary endpoint Tricuspid valve repair system (Abbott Medical Devices) TRILUMINATE (NCT03227757) Tricuspid regurgitation reduction ≥ 1 grade at 1 month
Composite of major adverse events at 6 monthsPASCAL (Edwards Lifesciences) Edwards CLASP TR EFS (NCT03745313) Freedom from device or procedure-related adverse events at 1 month TriCinch system (4Tech Cardio Ltd.) PREVENT (NCT02098200) Safety: The percentage of participants with major adverse events within 30 days of the procedure
Performance: The reduction in the degree of tricuspid regurgitation measured immediately after the procedure compared with baselineClinical Trial Evaluation of the Percutaneous 4Tech TriCinch Coil Tricuspid Valve Repair System (NCT03294200) All-cause mortality at 1 month TriAlign (Mitralign Inc.) PTVAS (SCOUT-II) (NCT03225612) Incidence of all-cause mortality at 30 days Cardioband (ValtechCardio) TRI-REPAIR (NCT02981953) The overall rate of major serious adverse events and serious adverse device effects at 30 days.
Successful access, deployment and positioning of the Cardioband device and septolateral dimension reduction intraprocedurally. Change in septolateral dimension at 30 days.Edwards Cardioband Tricuspid Valve Reconstruction System Early Feasibility Study (NCT03382457) Freedom from device or procedure-related adverse events at 30 days. MIA (Micro Interventional Devices Inc.) STTAR (NCT03692598) Safety: Major adverse event at 1 month
Performance: The technical success rate of MIA implant and reduction in the valve areaMIA = minimally invasive annuloplasty; PREVENT = Percutaneous Treatment of Tricuspid Valve Regurgitation With the TriCinch System; PTVAS = Performance of the Trialign Percutaneous Tricuspid Valve Annuloplasty System; TRILUMINATE = Clinical Trial to Evaluate Cardiovascular Outcomes In Patients Treated With the Tricuspid Valve Repair System; TRI-REPAIR = Tricuspid Regurgitation Repair With Cardioband Transcatheter System; STTAR = Study of Transcatheter Tricuspid Annular Repair
Source: Data from clinicaltrials.gov
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.