

A 41-year-old-male presented with a 1-month history of pruritic lesions on his scalp, neck, and penis. He had attempted a 2-week course of terbinafine cream, with no improvement. The lesions were unaffected by exposure to sunlight. The patient also reported new-onset wrist stiffness and pain. He had been diagnosed with primary syphilis 9 months prior to presentation, with a reactive plasma reagin titer of 1:64, and had been treated with intramuscular penicillin G benzathine 2.4 million units.
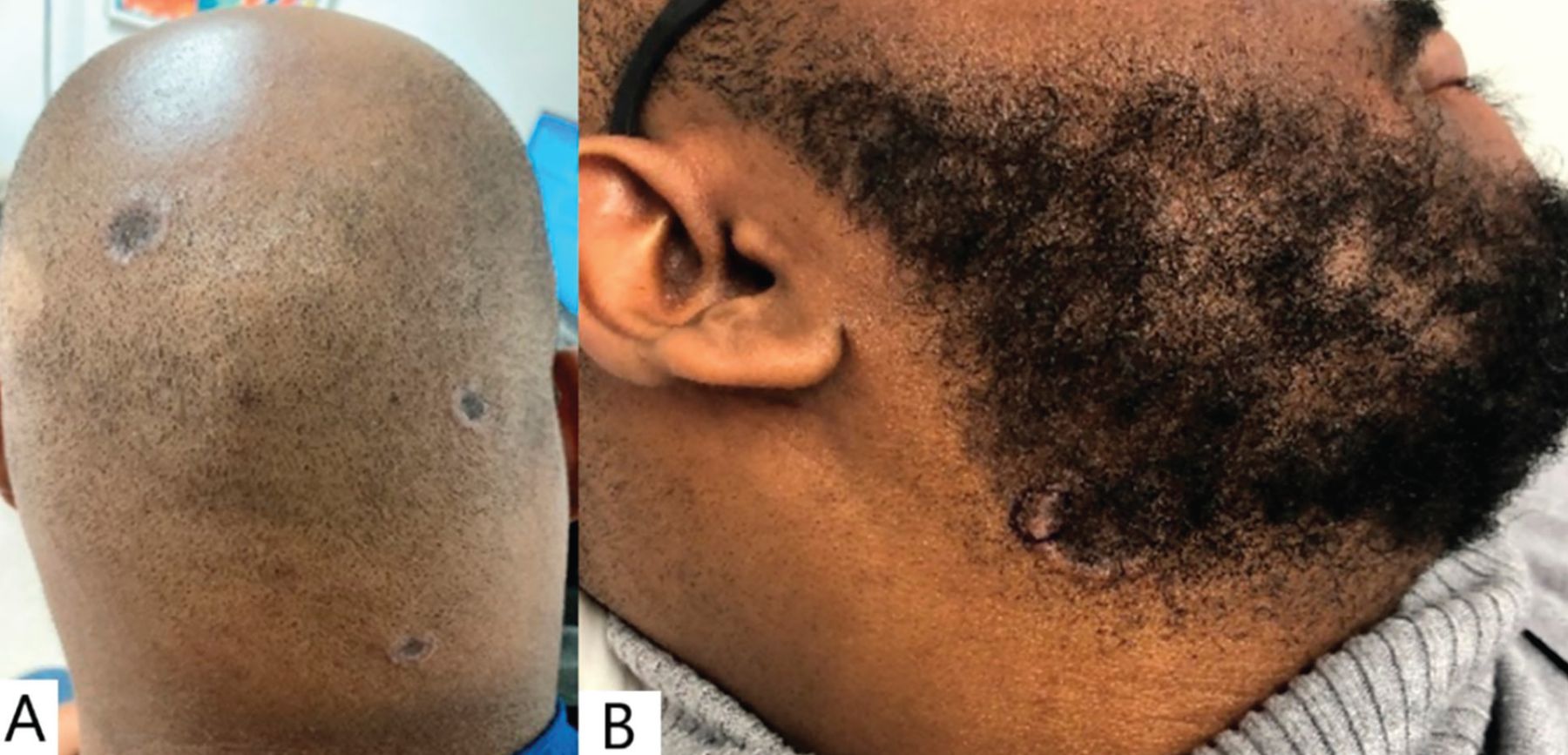
Physical examination revealed annular and petaloid plaques with central clearing and raised borders on the scalp, right mandibular angle (Figure 1), and penis (Figure 2). No lesions were observed on the oral mucosa, palms, or soles. No lymphadenopathy or new-onset alopecia was present.

The patient presented with annular lesions on the scalp and angle of the mandible. (A) Annular nonscaly plaques with central hyperpigmentation and a smooth, raised, pink border on the scalp. (B) Annular plaque with central hyperpigmentation, fine scale, and a raised, smooth, pink border on the right mandibular angle.

{kind=link}
{kind=link}
Subtle annular plaque (arrow) with central clearing and raised pink borders on the penis.
Clinically, the differential diagnosis included discoid lupus erythematosus, lichen planus, tinea infection, sarcoidosis, and annular secondary syphilis. Serology for human immunodeficiency virus was nonreactive, and cutaneous punch biopsy of the mandibular lesion was performed. Histologic sections revealed a brisk, mixed inflammatory infiltrate including numerous plasma cells within the superficial dermis to the mid-dermis. Staining for Treponema pallidum highlighted numerous spirochetes, consistent with syphilis. Repeat rapid plasma reagin testing was positive with a 1:256 titer.
Though not certain, we believed that this patient likely acquired a new case of syphilis after treatment of his previous infection, because he presented at 9 months after the primary diagnosis, and resolution of secondary syphilis typically occurs within 12 weeks.1 Therefore, he was given an intramuscular dose of 2.4 million units of penicillin G benzathine, with close follow-up recommended with the department of infectious diseases.
SECONDARY SYPHILIS AND OTHER PETALOID DERMATOSES
Clinical presentation
Syphilis is a sexually transmitted disease caused by the spirochete bacterium T pallidum. While primary syphilis typically presents as a solitary, painless papule or ulcer in the genital area, secondary syphilis is a generalized infection often accompanied by systemic symptoms such as fever, malaise, headaches, sore throat, or joint pain.1 These acute symptoms typically begin 6 to 8 weeks after the appearance of the primary lesion and resolve within 12 weeks.1
The most common cutaneous presentation of secondary syphilis is a generalized morbilliform rash, usually involving the palms and soles.2 However, secondary syphilis can present as annular secondary syphilis, which is also known as petaloid syphilis owing to its appearance resembling the petals of a flower.2 Lesions in annular secondary syphilis often occur close to the angle of the mandible and frequently spare the palms and soles.3–5 Secondary syphilis typically presents without lymphadenopathy and often affects the genitalia.5
MANAGEMENT OF PETALOID DERMATOSES
The differential diagnosis for annular plaques is broad and depends on clinical history, symptoms, and location and morphology of the lesions. Annular lesions on the head and neck could also be secondary to petaloid seborrheic dermatitis, tinea corporis, discoid lupus erythematosus, subacute lupus erythematosus, cutaneous sarcoidosis, or granuloma annulare.
A thorough history and physical examination, relevant laboratory studies, skin biopsy, and potassium hydroxide preparation of these lesions are helpful in narrowing the diagnosis.
TAKE-HOME POINTS
It is important for clinicians to consider petaloid secondary syphilis in the differential of annular lesions, as it can mimic other inflammatory and infectious etiologies.
DISCLOSURES
The authors report no relevant financial relationships which, in the context of their contributions, could be perceived as a potential conflict of interest.
- Copyright © 2023 The Cleveland Clinic Foundation. All Rights Reserved.