

A 45-year-old man with end-stage renal disease secondary to hypertension presented with abdominal pain, nausea, vomiting, and fever. He had been on peritoneal dialysis for 15 years.
Results of initial laboratory testing were as follows:
Sodium 137 mmol/L (reference range 136– 144)
Potassium 3.7 mmol/L (3.5–5.0)
Bicarbonate 31 mmol/L (22–30)
Creatinine 17.5 mg/dL (0.58–0.96)
Blood urea nitrogen 57 mg/dL (7–21)
Lactic acid 1.7 mmol/L (0.5–2.2)
White blood cell count 14.34 × 109/L (3.70–11.0).
Blood cultures were negative. Peritoneal fluid analysis showed a white blood cell count of 1.2 × 109/L (reference range < 0.5 × 109/L) with 89% neutrophils, and an amylase level less than 3 U/L (reference range < 100). Fluid cultures were positive for coagulase-negative staphylococci and Staphylococcus epidermidis.
Computed tomography (CT) showed diffuse parietal and visceral peritoneal calcifications encasing the small-bowel loops, consistent with encapsulating peritoneal sclerosis (Figure 1). His peritoneal dialysis catheter was removed, and he was transitioned to hemodialysis. He was discharged on a course of antibiotics and was started on prednisone and tamoxifen.

Computed tomography showed diffuse parietal and visceral peritoneal calcifications encasing the small-bowel loops (arrows), consistent with encapsulating peritoneal sclerosis.
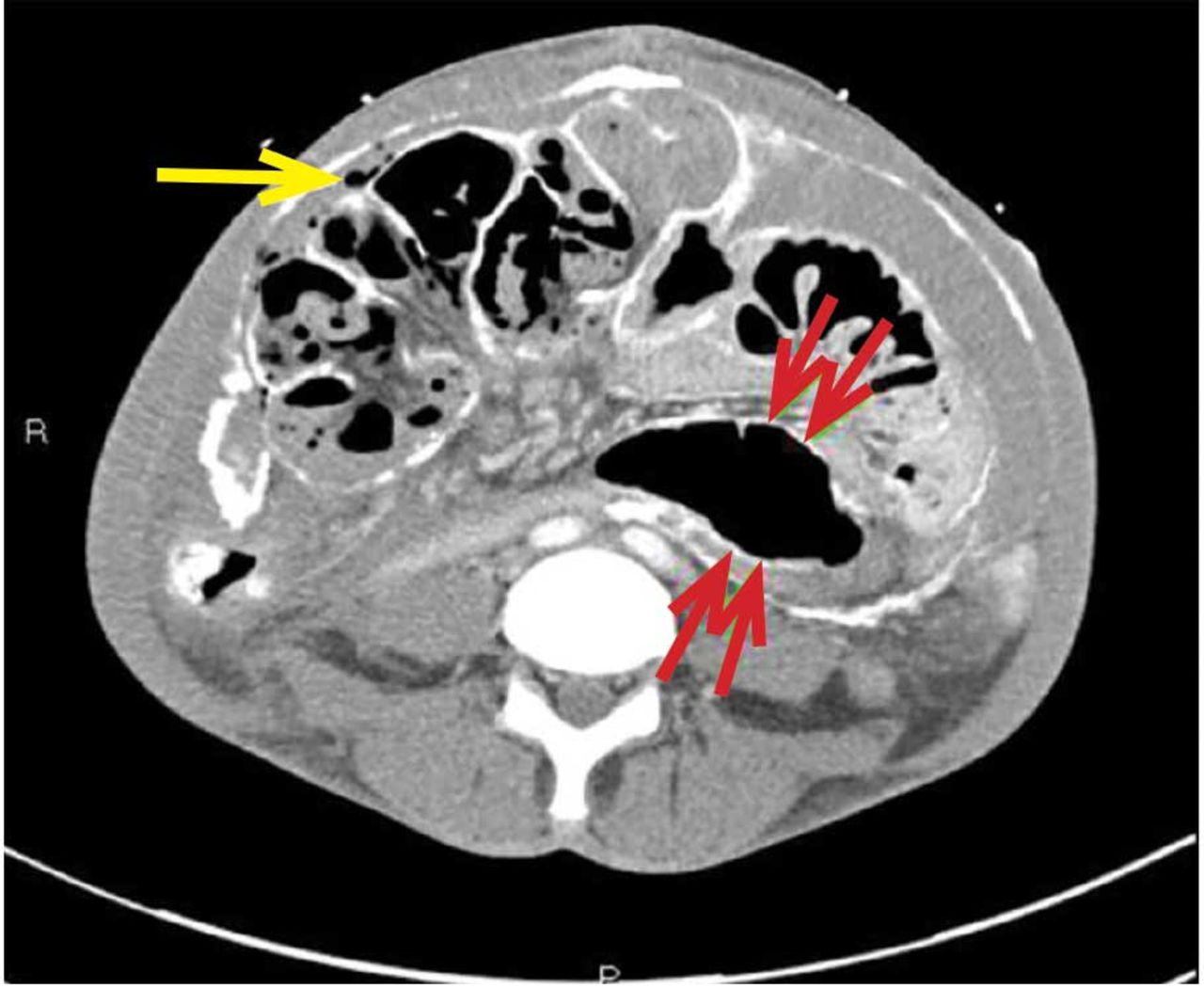
He presented again a few months later with abdominal pain. At that time, CT (Figure 2) demonstrated dilated small-bowel loops indicative of small-bowel obstruction and pneumoperitoneum consistent with bowel perforation. He declined surgical treatment and was referred for hospice care.

{kind=link}
{kind=link}
Several months later, computed tomography showed dilated small-bowel loops indicative of small-bowel obstruction (red arrows) and pneumo-peritoneum (yellow arrow).
CAUSES AND CLINICAL FEATURES
Encapsulating peritoneal sclerosis is a devastating complication of peritoneal dialysis, occurring in 3% of patients on peritoneal dialysis. The mortality rate is above 40%.1,2 It is characterized by an initial inflammatory phase followed by extensive intraperitoneal fibrosis and encasement of bowel. Causes include prolonged exposure to peritoneal dialysis or glucose degradation products, a history of severe peritonitis, use of acetate as a dialysate buffer, and reaction to medications such as beta-blockers.3
Clinical features result from inflammation, ileus, and peritoneal adhesions and include abdominal pain, nausea, and vomiting. A high peritoneal transport rate, which often heralds development of encapsulating peritoneal sclerosis, leads to failure of ultrafiltration and to fluid retention.
CT is recommended for diagnosis and demonstrates peritoneal calcification with bowel thickening and dilation.
TREATMENT
Treatment entails stopping peritoneal dialysis, changing to hemodialysis, bowel rest, and corticosteroids. Successful treatment has been reported with a combination of corticosteroids and azathioprine.4,5 A retrospective study showed that adding the antifibrotic agent tamoxifen was associated with a decrease in the mortality rate.6 Bowel obstruction is a common complication, and surgery may be indicated. Enterolysis is a new surgical technique that has shown improved outcomes.7
Footnotes
Dr. Geetha has disclosed consulting for ChemoCentryx and Genentech.
- Copyright © 2018 The Cleveland Clinic Foundation. All Rights Reserved.